Pharmacotherapeutic group: Drugs used in diabetes. Insulins and analogues for injection, intermediate- or long-acting combined with fast-acting.
ATC code: A10AD05.
Pharmacology: Pharmacodynamics: NovoMix 30 is a biphasic suspension of 30% soluble insulin aspart (rapid-acting human insulin analogue) and 70% protamine-crystallised insulin aspart (intermediate-acting human insulin analogue).
Mechanism of action and pharmacodynamic effects: The blood glucose lowering effect of insulin aspart is due to the facilitated uptake of glucose following binding of insulin to receptors on muscle and fat cells and to the simultaneous inhibition of glucose output from the liver.
NovoMix 30 is a biphasic insulin, which contains 30% soluble insulin aspart. This has a rapid onset of action, thus allowing it to be given closer to a meal (within zero to 10 minutes of the meal) when compared to soluble human insulin. The crystalline phase (70%) consists of protamine-crystallised insulin aspart, which has an activity profile similar to that of human NPH insulin.
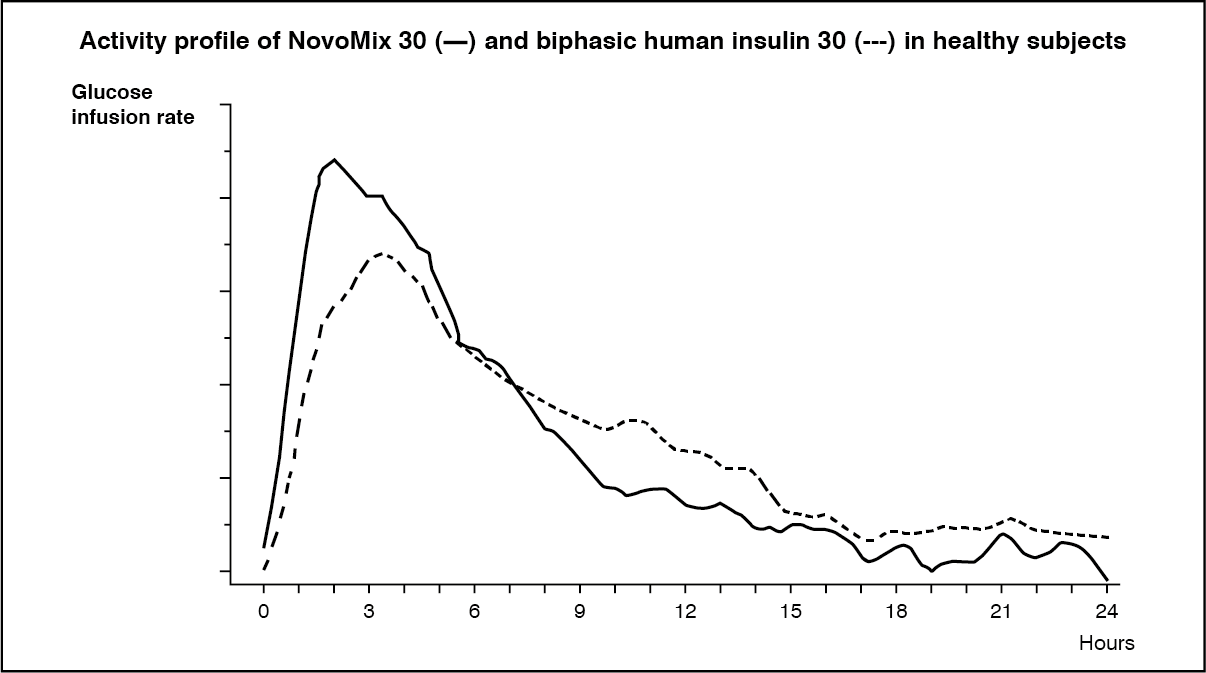
When NovoMix 30 is injected subcutaneously, the onset of action will occur within 10 to 20 minutes of injection. The maximum effect is exerted between 1 and 4 hours after injection. The duration of action is up to 24 hours (figure). (See figure.)
 Click on icon to see table/diagram/image
Clinical efficacy and safety:
Click on icon to see table/diagram/image
Clinical efficacy and safety: In a 3 month trial in patients with type 1 and type 2 diabetes, NovoMix 30 showed equal control of glycosylated haemoglobin compared to treatment with biphasic human insulin 30. Insulin aspart is equipotent to human insulin on a molar basis. Compared to biphasic human insulin 30, administration of NovoMix 30 before breakfast and dinner resulted in lower postprandial blood glucose after both meals (breakfast and dinner).
A meta-analysis including nine trials in patients with type 1 and type 2 diabetes showed that fasting blood glucose was higher in patients treated with NovoMix 30, than in patients treated with biphasic human insulin 30.
In one study, 341 patients with type 2 diabetes were randomised to treatment with NovoMix 30 either alone or in combination with metformin, or to metformin together with sulfonylurea. The primary efficacy variable - HbA
1c after 16 weeks of treatment - did not differ between patients with NovoMix 30 combined with metformin and patients with metformin plus sulfonylurea. In this trial, 57% of the patients had baseline HbA
1c above 9%; in these patients, treatment with NovoMix 30 in combination with metformin resulted in significantly lower HbA
1c than metformin in combination with sulfonylurea.
In one study, patients with type 2 diabetes, insufficiently controlled on oral hypoglycaemic agents alone, were randomised to treatment with twice daily NovoMix 30 (117 patients) or once daily insulin glargine (116 patients). After 28 weeks of treatment following the dosing guideline outlined in Dosage & Administration, the mean reduction in HbA
1c was 2.8% with NovoMix 30 (mean at baseline = 9.7%). With NovoMix 30, 66% and 42% of the patients reached HbA
1c levels below 7% and 6.5%, respectively, and mean FPG was reduced by about 7 mmol/l (from 14.0 mmol/l at baseline to 7.1 mmol/l).
In patients with type 2 diabetes, a meta-analysis showed a reduced risk of overall nocturnal hypoglycaemic episodes and major hypoglycaemia with NovoMix 30 compared to biphasic human insulin 30. The risk of overall daytime hypoglycaemic episodes was increased in patients treated with NovoMix 30.
Paediatric population: A 16-week clinical trial comparing postprandial glycaemic control of meal-related NovoMix 30 with meal-related human insulin/biphasic human insulin 30 and bedtime NPH insulin was performed in 167 patients aged 10 to 18 years. Mean HbA
1c remained similar to baseline throughout the trial in both treatment groups, and there was no difference in hypoglycaemia rate with NovoMix 30 or biphasic human insulin 30.
In a smaller (54 patients) and younger (age range 6 to 12 years) population, treated in a double-blind, cross-over trial (12 weeks on each treatment), the rate of hypoglycaemic episodes and the postprandial glucose increase were significantly lower with NovoMix 30 compared to biphasic human insulin 30. Final HbA
1c was significantly lower in the biphasic human insulin 30 treated group compared with NovoMix 30.
Pharmacokinetics: Absorption, distribution and elimination: In insulin aspart, substitution of amino acid proline with aspartic acid at position B28 reduces the tendency to form hexamers as observed with soluble human insulin. The insulin aspart in the soluble phase of NovoMix 30 comprises 30% of the total insulin; this is absorbed more rapidly from the subcutaneous layer than the soluble insulin component of biphasic human insulin. The remaining 70% is in crystalline form as protamine-crystallised insulin aspart; this has a prolonged absorption profile similar to human NPH insulin.
The maximum serum insulin concentration is, on average, 50% higher with NovoMix 30 than with biphasic human insulin 30. The time to maximum concentration is, on average, half of that for biphasic human insulin 30. In healthy volunteers, a mean maximum serum concentration of 140 ± 32 pmol/l was reached about 60 minutes after a subcutaneous dose of 0.20 unit/kg body weight. The mean half life (t½) of NovoMix 30, reflecting the absorption rate of the protamine bound fraction, was about 8-9 hours. Serum insulin levels returned to baseline 15-18 hours after a subcutaneous dose. In type 2 diabetic patients, the maximum concentration was reached about 95 minutes after dosing, and concentrations well above zero for not less than 14 hours post-dosing were measured.
Special populations: The pharmacokinetics of NovoMix 30 have not been investigated in elderly patients or in patients with renal or hepatic impairment.
Paediatric population: The pharmacokinetics of NovoMix 30 have not been investigated in children or adolescents. However, the pharmacokinetic and pharmacodynamic properties of soluble insulin aspart have been investigated in children (6-12 years) and adolescents (13-17 years) with type 1 diabetes. Insulin aspart was rapidly absorbed in both age groups, with similar t
max as in adults. However, C
max differed between the age groups, stressing the importance of the individual titration of insulin aspart.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity and toxicity to reproduction and development.
In
in vitro tests, including binding to insulin and IGF-1 receptor sites and effects on cell growth, insulin aspart behaved in a manner that closely resembled human insulin. Studies also demonstrate that the dissociation of binding to the insulin receptor of insulin aspart is equivalent to human insulin.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out